Through Tongue Tie Babies Support Group, I "met" Jen, and then we were able to meet in real life. While Ezra and I struggled with common tongue-tie issues related to excessive weight gain, reflux, "oversupply," and all with a happy baby, Jen and Christian were at the other end, experiencing intense colic, nursing around the clock, failure-to-thrive, reflux, and diminished milk supply. I asked her to share her story, and it is extreme. I am grateful for her willingness to upturn all of these feelings and emotions, and I know she does it to help other families.  A few days old, sticking his tongue out A few days old, sticking his tongue out Even though it has already been six months since we went through our revisions, I still find it hard to think about what my son Christian and I went through with his undiagnosed tongue and lip ties. I should include my husband, Scott, in that statement as well, as he had to be there for all of the problems we were dealing with. He spent his time home with us soothing a screaming baby -- a baby who we thought had reflux, gas, and colic. He helped me cut out every offensive food in my diet that could have been making him sick (according to all of our baby books and the websites I read, Christian was probably upset all the time because of my diet, the gas that infants naturally have, and because he was just a “colicky” baby). For his first two months of life, we spent 8-10 hours a day laying on the couch nursing. He would
fall asleep a few minutes in, and I would try to get up to do something around the house or grab a bite to eat. As soon as I moved, he would scream until I nursed him again. I would see a little heart-shape at the end of his tongue and a piece of tissue going halfway up his tongue that I thought was suspicious, but I didn’t think too much of it.
Let me backtrack. I was supposed to have Christian in a birth center until we had complications three days into my labor. He went from the right position to the wrong position and I couldn’t dilate due
to horrible back labor. I was not planning on spending time in a hospital, but during our overnight stay I must have called the nurses every hour to help me with breastfeeding a baby that couldn’t latch well from the get-go. I was told that not being able to latch was normal and we both had a lot to learn with each
other. The advice didn’t sit well with me because it seemed extremely hard to breastfeed him. A nurse supplied me with a nipple shield and we “kind of nursed.” It still hurt, but I had a tool that helped a little.
I left the hospital with my baby and my shield promising to appear at our pediatric follow-up the next day. When Christian was weighed, we saw that he went from 8lbs 5oz to 7lbs 12oz overnight. The doctor
didn’t seem concerned and arranged for us to come back a few days later -- he was barely at 8lbs at that visit. She said that since he was gaining weight, even though not quickly enough, she wasn’t too worried and I should just come back in for our two month appointment. She chalked up the weight loss as being a normal symptom of jaundice and that some time in the sun and feeding him constantly would clear him of it.
 Newborn Newborn We spent the next seven weeks nursing all day and all night. I had bruised nipples and the baby had blistered lips. I had heavy letdowns in the morning and he would spit up most of what he drank. I was irritable, frustrated, and would spend the five minutes a day I had alone crying in the shower. My husband learned all kinds of tricks to calm the baby, although now I’m realizing that we made him cry it out and he just gave up and slept because he realized he wouldn’t get any food. That’s my best guess, anyway. I don’t think our gas moves were helping him. Being new parents, we figured that we had to work out the gas and when he would fall asleep we figured we did our hard jobs as parents. We had no idea how hungry he was.
 2 months 2 months When two months rolled around, Christian looked really thin and I started to worry about him. His head was huge, his arms were tiny, and I could see his ribs clearly. My best friend said he didn’t look any bigger (but I didn’t notice how skeletal he was until I looked at pictures I had taken). She noticed him falling asleep while eating and thought he didn’t have a deep latch.
I heard of a breastfeeding group that was part of a local hospital and I decided to go in for support to figure things out. The first time I went, the lactation consultants thought he was a newborn. When they saw him eat, then told me that he was just a lazy baby and they see lazy babies all the time. I was told to constantly make him uncomfortable so that he would
eat. They said he was “happy to starve” and he “circled the drain” -- whatever that meant. Basically, they told me that he preferred just to eat enough to be comfortable and then go to sleep (from my own research, I found that he was working so hard at eating that he fell asleep out of exhaustion). No mom wants to hear these words about their child and instinctually, the situation didn’t
sit right with me. I showed her the ties and wanted her confirmation that they weren’t normal (at that point I read a little about posterior tongue tie and upper lip tie in the Facebook Tongue Tie Babies Support Group) and she told me that they were normal, they see them all the time, and that they would stretch. She told me that my bruises were normal and his lip blisters were normal. I wanted her to tell me what my gut was telling me: the ties were the problem. Instead, the baby was blamed. Unfortunately, he was diagnosed failure-to-thrive by the lactation consultant who told me to go see the pediatrician right away or else they would make sure he would be admitted to the hospital. I was told to take fenugreek, pump, and give him as much formula as he would take.
 2 months 2 months When we went to his pediatrician, she told me that he was fine, not yet failure-to-thrive, and I probably just didn’t make
enough milk for him. I pointed out his posterior tongue tie and upper lip tie and she said that those are normal and they would stretch in time. Both pediatrician and lactation consultant agreed I should rent a hospital-grade pump and pump/bottle feed for every single feeding. The lactation consultant sent me home with a case of formula since I probably didn’t have enough milk for him and by that point, she was right. We had two months of bad latching and
breastfeeding and my milk supply, although there, was hardly established. I went through the next month pumping, bottle feeding, and “sneaking in” breastfeeding sessions to make sure we kept our closeness and he didn’t decide the bottle would be better for him.
As if pumping, bottle feeding, charting weight and diapers (we bought an infant scale and weighed him six times a day) weren’t enough, there was a huge strain on me feeling like a failure. I could not wrap
my mind around my baby being lazy and happy to starve. My instincts were telling me that this baby would do anything he could to survive, and that something had to be an issue. I originally found out about the Tongue Tie Babies Support group through another breastfeeding site where many of the moms were also telling me that all of these things were normal and that we would just work through them. I was told to take fenugreek, eat oatmeal, have a beer, drink a ton of water, and try all kinds of positions. Where some of these things helped a little, I thought they were more like bandages and not cures. After reading through most of the posts, I came across one from a mom who described my story exactly: feeding the baby all day, baby falling asleep, waking up crying, gas, colic, reflux, failure-to-thrive.
She spent the next few hours communicating with me back and forth and encouraging me to go to the support group. There, other parents were telling me almost the same exact story. When I asked why I was told it was my fault or my baby’s fault, they explained that doctors and lactation consultants usually aren’t taught these things in school. I read Dr. Kotlow’s breastfeeding publication and looked through all of the articles I could get my hands on. Finally, the mom who originally linked me with the group told me to go see Dr. James Jesse who only lives an hour away. I made an appointment for the first available opening which was a week away. When I went to tell my midwife, she told me to see someone closer to us and although I agreed, I kept my appointment with Dr. Jesse.
When I saw the pediatrician who clips lip ties, she told me that his tongue tie was very minor and although she would clip it, it probably wasn’t really causing us that many problems. She said his upper lip tie was “too thick” to clip and that I should just wait until he broke it on his own or was old enough to go under general anesthesia and could have it stitched. She watched him eat a bottle and told me that I could just bottle feed him, but I probably just wanted the closeness. As a mother determined to breastfeed, yes, I wanted closeness. I wanted so much more than that. Her lack of knowledge and
incomplete revision (both of not revising the upper lip tie and also not cutting enough of the tongue tie) discouraged me but the support group assured me that Dr. Jesse would take care of both issues. When I called his office to confirm, the receptionist said that there wasn’t a tongue or lip tie Dr. Jesse couldn’t take care of.
 Getting chubby! Getting chubby! I took Christian into see Dr. Jesse and within ten minutes he was diagnosed and revised via laser. I couldn’t believe the
difference I saw in his mouth, and although he had a hard time breastfeeding right away, he ended up napping which gave me time to allow him to heal.
Our story didn’t end with the revision. After a traumatic birth and two months of bad and overcompensating latch, we had
Christian go through craniosacral therapy and chiropractic adjustments. After working with him on his latch and suck, we finally have a good, pain-free breastfeeding relationship. Sometimes I think his suction is a little too good -- creating quite a seal when he latches. I never saw or felt that before when he had posterior tongue and lip tie! After trying an SNS for feedings, I couldn’t really get the hang of it and decided to opt for bottle feedings for supplementing. Some women can boost their milk supply up in big ways after revisions, but mine never quite got to where it needed to be. He wasn’t gaining enough weight still and so I had friends who donated over 150oz of breastmilk to me and we found a formula that he liked. I have to say my milk supply did increase a lot, and with that I have been able to go from supplementing 15-20oz a day to 0-6oz a day, depending on Christian’s needs. He has been gaining weight steadily and his gas and reflux have not been an issue since his revisions. I haven’t worried about the types of foods I eat, nor would I label him colicky. We even took a trip to Colorado for a friend’s wedding when he was three months old and he was not the same frantic baby he was at one or two months old. I enjoyed his first laugh without looking at the fragile, skeletal sweetheart that I would have done anything for.
 Christian, 7 months old Christian, 7 months old Even though he is currently behind in weight (tenth percentile), he is healthy, happy, growing, and meeting major milestones. I am just following his lead in providing for him, and it is working out well without a lot of stress. We know that one day this will really be behind us with Christian. We know that we will take our next babies in for revisions as early as a day post-birth if they have ties, and chances are, they will. When I went back to visit the lactation consultant I worked with, she didn’t seem to want to listen to our story, but I plan on going back in with information and resources hoping that she and her colleagues will see this common problem that many moms face and learn the ways they can support them so that no baby will ever be called lazy again. Because of our experience, I want to save other moms the pain of going through what we went through with an issue that is so easily diagnosable and treatable. I hope that my friends can learn from our experience and realize that with their similar issues, their doctor may not have all the answers. I am also thankful that I was proactive in preventing adult issues with tongue and lip tie such as speech problems, digestive issues, tooth decay, and other symptoms that I struggle with as an adult as I have an undiagnosed posterior tongue tie myself.
Even though having a baby diagnosed as failure-to-thrive is devastating, I am thankful for going through the extreme end of the issues because I can use our experience to help other mothers who are struggling. I don’t regret the revisions at all, and would do it all again in a heartbeat knowing that it is fully benefitting Christian.
 Through the ACA, insurance companies are required to cover a breastpump for women who have nursing babies. I am not going to get all law-tech-bureaucratic on you, but since I recently went through the process and have had a lot of inquiries on how it worked for me, I thought I would share my experience. It is my understanding that even though this is something insurance companies are "required" to offer, the follow-through is what varies from company to company. Some only allow a manual breastpump; some allow a higher-quality, hospital-grade pump if your baby was premature. Still others set the fee of what they will cover, and if you go over that with upgrades or a higher-level pump, the difference is yours to pay. After Ezra was born in April and we were dealing with his tongue and lip ties (which I wasn't aware of yet), I called my insurance company (Anthem Blue Cross) to see about getting a pump. They gave me the information for two DMEs (durable medical equipment suppliers). I was in a lot of pain and experiencing a lot of engorgement. I was desperate! I called one company, and even their hold message stated they were backed-up for pump orders. I hung up and called the other DME. After some waiting, I got through. They only offered two pumps: Playtex and Medela. Coming from a breastfeeding advocacy background, this wasn't good to hear. My issue with Playtex: We often counsel women not to buy pumps from companies that make bottles -- the research and science isn't there when it comes to putting together a breastpump that works well. My issue with Medela: They are no longer WHO-code compliant ( easy to understand info here), and while that isn't the biggest deal to some, it is something very important to me. After a lengthy conversation, exchange of a lot of information, and a hot cell phone to my head (hot baby to my chest, hot engorged breasts), I chose the Medela pump. I waited a week, and after not hearing from anybody, I called the DME to see what the status was. I was told I needed to pay around $80. Now I had been told by my insurance company I would pay 20%, so $80 for a $250ish pump seemed wrong to me. I talked to someone else in some other department, and she said they would look into it and get back to me. What really must have happened was, the order got cancelled, because I never got a breastpump, and they never got back to me. But by then, I was feeling much better and we had worked some of our issues out. Fast forward to about a month ago. I was at a LLL meeting and a mother said she had just ordered a Hygeia pump through her insurance and they covered the whole thing at 100%. I then learned, we had the same insurance! This was her advice: Contact Hygeia directly and tell them you want their pump. I did, and a week later, I got my pump, nothing paid out of pocket, and I already have some milk in the freezer! Not everyone's process will be that easy. It is worth a try, though. My understanding is, you have from your third trimester until your baby's first birthday to get a pump. I didn't think about getting one before birth because I have been trained and ingrained to counsel women NOT to buy pumps while pregnant. It is often on that baby registry -- a Medela Pump in Style (PIS). With my childbirth ed classes I have suggested, if a woman isn't going back to work or school immediately, to hold off on buying a pump. With more time and a meeting with an IBCLC, often a women can better determine what type of pump will fit her needs best, versus the PIS simply because that is the one she has heard of, and her sister/best friend/next door neighbor used it, and maybe even someone is giving her their old pump, so she's set. The thing about the PIS is, it is not the best pump out there -- like we say about carseats, the best carseat for your child is the one that best fits your child AND your car. Same with pumps. The best pump is the one that best fits you, not only physically (nipple size) but also functionally (are you going back to work or will you just need some milk for date night?). Pumps are pricey...they aren't always something needed before a baby is born. In the beginning, mom and baby are supposed to be determining how the relationship goes, how to latch, how often to feed, how much milk, etc. The pump, under normal circumstances, doesn't need to be a part of that early relationship. If a woman finds herself pumping, it is often because there are some adjustments needed due to soreness or pain, and that is where a LLL Leader or IBCLC can come in handy. If you have a premature baby, or a baby who is unable to latch, of course a pump is what you need to protect the milk supply until baby can return to the breast, so don't think I am saying it always goes smoothly -- I know it doesn't. In situations like that, though, a hospital-grade pump, which needs to be rented, is almost always going to be a better choice, so you still wouldn't miss out if you hadn't purchased a pump before birth. Back to the giving-away-of-the-old pump: I admit, I used my sister-in-law's pump 14 years ago, when my baby was in the NICU for two weeks, and I was grateful to have it. I knew nothing about pumps, barely anything about breastfeeding. At that point it had been used for three of her babies, and I am sure it had logged many, many hours. I don't worry that I could have cross-contaminated my milk in there (the PIS is an open-system, which means milk could potentially get into the motor and come in contact with the next mom's milk), but I probably should have worried about the potential for mold growth and my sick NICU baby's health, or even bugs that can get into the motor(yes, cockroaches can visit and maybe even stay). Pumps are so expensive, though, it isn't unusual for us to want to share them when we are done, or to even sell them to strangers. Please, don't. Not if your pump is designed as a single-user item -- treat it like nose-hair trimmers -- you wouldn't share those with anyone, would you? Hygeia knows when you spend so much on something and it still has life left, you are likely to share it -- and their closed-system allows this simply by having the next woman purchase her own pump parts -- the tubing, the flanges, the storage containers. Ameda ( WHO-code violator) also makes a closed-system pump. Bailey is another great quality, lesser-known company that makes pumps. Like I said before, just because Medela is the best-known, doesn't mean they are the best for you. Once you decide you want a pump, check out who your insurance company's DMEs are; if they have a pump you like, then go for it. If you want more choices, try contacting the pump company directly to see what DME they suggest. I just have to say: The amount you can pump does not determine how much milk you have -- some women don't respond well to pumps, that is a fact. If you need help pumping or breastfeeding, contact someone -- you don't have to figure this all out on your own. LLL Leaders can answer questions and provide information about how to pump more successfully, and a personal consultation with an IBCLC can be invaluable when you are tying to figure out the hows and whys and whens of pumping when you are getting ready to go back to work -- they are a wealth of information. I do not have any relationship with Hygeia, I am just super-impressed with the measures they take to make their pumps relevant in a market where $200 pumps could essentially be tossed in landfills if they were truly being used properly. I would love to hear about your experiences with obtaining a breastpump through the ACA.
 You know how they say, “Wear sunscreen? Well, let me be your cautionary person-writing-this-blog-post and say, up front, WEAR YOUR SUNSCREEN. On that note of “The more you know” (did you just hear the music?), let me also share that we need to watch our skin for more than just those changing moles we always hear about. Yesterday I had a Mohs procedure on a superficial basal cell
carcinoma on my face (yes, skin cancer). My only clue this was something that needed attention was the fact that, all summer, I had this spot on my nose that would scab up for a week or so, and then heal. Scab, then heal. Scab, then heal. It was a shiny piece of flesh-colored skin that maybe looked a bit callused – no pigmentation, no mole appearance, just a regular area of skin that looked and
behaved a little differently. A visit to my dermatologist revealed it was problematic, and that leads us to the Mohs procedure.
In order to fully get the root of the tumor, a Mohs surgery can be lengthy. The skin is numbed, the surgeon draws, and then they cut. They take that piece of tissue and essentially put a cross-hair on it,
mapped to match the area from where it was removed. This is examined to see if all the bad cells are gone (I never said I was an expert). If they see anything remaining on the sample, they know exactly where the offending tissue lies; my surgeon had to come back one more time in true, if-at-first-you-don’t-succeed fashion. There is a wait time of 30 minutes between each sample, which is why this isn’t generally an in-and-out procedure.
After this was all taken care of, I expected my doctor would just swab some antibiotic ointment and slap a cutesy Band-Aid on and that would be it. But I was wrong. I actually had to go to a different part of the building. “I’ll meet you over there, “ my handsome, thirty-something, Mediterranean (Middle-Eastern? Spanish? Who knows) hunky doctor said. Then a nurse walked me through some doors, shoved some things into my arms, and said, “Go ahead and put your clothes in the bag.” Um, what? I am just getting
my nose bandaged!? What’s going on?
In the shock of suddenly realizing I needed to strip down, I couldn’t remember if the gown was to open in the front or the back. I tried it one way, spun it around, then twisted it back the first way. Finally with it half on, fabric clenched in my hands to cover my behind, I stuck my head out to call, “Hey, what’s the story on the gown? Open in the front or the back?” The back, definitely the back.
I continued with my booties and the ever-lovely surgical hair-net thing. I was placed in a bed and my nurse brought me a warm blanket -- other accoutrements included an automatic blood pressure cuff, and a pulse ox on my right index finger. My nurse sat and chatted with me for a bit, over such everyday topics as allergies to any drugs (none), was I supposed to take my bra off, because I did (there are so few places outside of one’s own home where I can do this, so why not? But no, it was not required), and the fact that we both were breastfeeding mothers (can’t remember how that came up).
I was actually wheeled, wheeled, I say! into the surgery (that sounds so Doc Martin, but unlike the European definition, this was the place in the surgery center where they do surgeries, not the office where docs do visits). When my doctor came in, I was kind enough to remind him that it had been a couple hours since last my nose was bee-stinged beyond feeling, so I would love some more drugs to numb that region. Here is the comment that started it all: “I think I have a pretty high pain tolerance, but I don’t want to feel this if I don’t have to.” His response was, “Oh, why do you think that?” I shared I had 4 babies with no pain meds. He and the two nurses all gasped. Oh, I had one more coming, “And the last one was born at home.” My nurse fainted to the floor.
Okay, not really. But I they were still abuzz with a lot of questions, that all sounded like “Why?” (Let me come down off my high-horse now.) “I wasn’t planning to have my first without pain meds. In fact, I said, ‘I have seen women give birth naturally, I think it’s pretty crazy; I am totally getting an epidural.’ Well fast-forward to an unneeded induction, and I wasn’t able to get an epidural. My fear of throwing up won out over my fear of having a baby, so I somehow was able to give birth to my first baby without an epidural or narcotics. It took some time to work through mentally, but eventually, I was happy about
it.”
 By this time in the surgery, my bed has been lifted up, the doctor has cleaned the left, upper quadrant of my face with iodine, my eyes stinging from the closeness of the fumes, and my face has been covered with a piece of paper with a circle cut out of it so only my nose is exposed.
I continued on…“With my second baby, I wondered what could birth be like if I actually planned to not use any medications? I got a midwife who delivered in the hospital, and I waited to go into labor on my own. Third baby, the same. Fourth baby, we moved here, there were no hospital-based midwives, so I found a licensed midwife who came to our home to help us have our baby there.”
“Why would someone choose to not have pain medications? It is painful to have a baby!” he stated, with much authority (at this point, I did question how he knew this, had he ever experienced it? To which
he conceded, no, but he had seen it a lot). So I asked him this: “Why would someone choose to climb Mt Everest?”
“That’s different,” came his reply, “I can understand that. You want to see what you are able to
accomplish physically. You are challenging your body, working toward a goal...” My pulse-ox’d finger interrupted him, pressing, pressing on its imaginary quiz-show buzzer – or maybe it was my voice -- “DING DING DING! You got it!”
I couldn't see him because my face was covered, but his hands paused in their stitching. “I…could see that,” he came around, slowly. The hands resumed their stitching. “I am not sure what the big deal is about drug-free birth though. There is so much pressure to have a natural birth, but we don’t have the
longitudal studies that show epidurals, or even c-sections, have life-long health risks.” On the spot, under the cover of plastic-y-paper, I couldn’t think of anything incredible to counter with. I did cite that babies born via cesarean birth have higher levels of allergies, and that was about all I could think of.
I joined him, then, because I do feel it’s the truth, “There is a lot of pressure for women to go all natural, I see that. It is very similar to the pressure we put on women to breastfeed -- ” Okay, this is when he cut me off!
“ – But those stats are there, we know breastfeeding is beneficial, we have that information.” Interesting!
Super, hard-cord breastfeeding advocate, not so much on the normal birth platform! I decided, since I
couldn’t present any compelling evidence-based studies or data from Cochrane, I would just keep it simple and stick with his line of thinking. “We are humans, though, and we know as mammals, breastmilk is the optimal, species-specific diet for our newborns.” He agreed. "Doesn’t it stand to reason, then, that
vaginal birth, as unhindered as possible, is the norm for us as well? And even though we have the option for epidurals and cesarean births, that vaginal birth would provide the most optimal way for our babies to be born?” Honestly, I can’t remember what he said after that, only I know he wasn’t trying to refute anything.
The cover was lifted off my face and it was time for the nurses to step in and dress my wound. As he stepped back to let them take over, he asked, “Are you a medical professional?” I paused before my
answer, and then said, “No, I am a birth doula, a childbirth educator, and a La Leche League Leader.” He shook my hand, nodded his head to me, and then departed to fill out my discharge papers.
What fun! It made all those 5 bee stings to the nose worth it. I can actually say, due to that conversation, I rather enjoyed my day at the dermatologist. The staff was incredible and attentive (and I am assured my scar will be minimal). You never know where great birth conversations will happen! But the opportunity to have 20 minutes, one-on-one with a surgeon (albeit a derm surgeon), was pretty darn fun.
 Ezra listening intently as Dr. Jesse explains the procedure Ezra listening intently as Dr. Jesse explains the procedure We decided to see Dr. James Jesse in San Bernardino, CA. It was a four hour drive for us, and to ease the stress of travel, Brad, Ezra, and I drove down the day before and stayed in a hotel. During my Virtual Adventures in Tie-Land, I met a LLL Leader and IBCLC who lives about an hour south of me, Julie Huisjen. She was the one who really planted the idea of visiting Dr. Jesse and seeking laser revision for the ULT and PTT, as opposed to scissors for the PTT alone. As much as I didn’t want to travel that far, I came to the realization that a trip to Dr. Jesse was the way to go. As a bonus, Julie asked if she could come and observe the procedure, and I was pleased for the opportunity to meet her and have additional support. Julie was waiting for us when we arrived at the office, and although we just met, I was grateful for her presence. When Dr. Jesse came to our room he was friendly and up-beat. He examined Ezra and agreed that we could benefit from having the ties revised. He explained the procedure, answered questions, and was appreciative of Julie’s and my breastfeeding background.
 Ezra's laser action Ezra's laser action I sat in the dental chair with Ezra’s head on my left shoulder. I held my arms over Ezra’s chest, thereby pinning his arms but allowing his feet freedom to kick. Dr. Jesse numbed Ezra’s mouth, and then we sat and chatted for a few minutes to allow the anesthetic to take effect. Dr. Jesse was very personable with a great sense of humor. We asked to video the procedure and Dr. Jesse welcomed it -- that way I could watch it later.
Two assistants helped, one holding Ezra’s head behind us, and another to the right of us who was holding the spit-sucker (I am sure there is a technical term for that!). Once started, the actual procedure took less than 5 minutes. Ezra cried and moved a lot, but I knew he was probably more bothered by the restraining of his head than the laser surgery happening in his mouth. There was a little blood to be blotted with gauze, and that was it!
 All done! All done! I sat up and looked at my fat-lipped baby as Dr. Jesse said, “From here on out things will get better.” I asked how soon I could nurse him, and smiling Dr. Jesse answered, “Moms like you nurse right away.” We tried, but Ezra’s numb mouth made latching difficult. I decided we would try again later. Dr. Jesse said babies cry for about 8 minutes post-revision, and then they are usually okay. We happened to have the appointment before lunch, and Dr. Jesse was kind enough to talk to us for another 30 or 40 minutes, generously sharing information, stories, and jokes.
 Getting ready to try and nurse Getting ready to try and nurse We went to lunch and I nursed Ezra for the first time. I could already see a part of his upper lip turned out that I had never seen before – it wasn’t a huge flanging or anything, but it was something. I didn’t notice relief, though – if anything it felt a little tighter (read: worse).
Ezra was acting fine when we hit the road and headed for home. 30 minutes from home he began crying inconsolably. We stopped at Costco and I tried to nurse him in the car. He would attempt to latch, but then he acted like his mouth hurt (which I could believe!). I was worried about him not nursing, but they told me at the office he might not want to nurse too much in the first 24 hours, so it wasn’t a surprise. I decided at that point to give him Tylenol, we walked around Costco for about an hour, and then he settled down to nurse. I still couldn’t tell a difference in my pain level.
 Melting into his cousin Caleb Melting into his cousin Caleb I gave him one more dose of Tylenol later that evening, and by the next afternoon, he seemed back to normal. Dr. Jesse’s office instructed us to stretch the upper lip and sweep under the tongue once every hour Ezra was awake. We went to a chiropractor the next day, and I have never seen Ezra so melty afterwards, if that’s a word. Ezra’s “reflux” stopped almost overnight. He would still spit up, but it was nothing like it had been before. His clicking was mostly gone. That strange (cute) way he had of chewing up to latch on the nipple with a grimace on his face was gone, as was his way of sliding off the nipple while nursing. He seemed to be doing better, but I was still waiting… Sometimes he didn’t mind the stretching, other times he hated it. One thing I figured out was to do the stretches as far away from a feeding session as I could, or we might have a hard time nursing afterwards. One week passed and although Ezra seemed happy, I wasn't noticing anything much more than not having to hold the breast for him every time he nursed. I am so grateful for Tongue Tie Babies Support Group, there I received realistic ideas about how things might shape up for us over time. Although some women note instant relief after their babies' revisions, it seemed to me for every one who had that experience, there were 4 women who said it took many weeks for full effect. If I hadn't known that, I would have felt the surgery was a waste of time and money. So I kept up with the exercises and tried to encourage wider and deeper latching. Speaking of money, in my haste to get this done I didn't ask Dr. Jesse's office the price of the procedure or what my insurance might cover. As Ezra was a newborn, I hadn't thought to sign him up on our dental plan, which would have covered the surgery. I was surprised to have to pay out-of-pocket for the surgery -- it was $400. I was happy to do it (although I will be even happier if our medical insurance reimburses us some!). Realistically, that is an affordable price for this procedure, in my opinion. Two weeks passed and I wasn't feeling better. The nipple shape still showed some compression stripes after nursing. Before the revision, it was more painful to nurse on the left side; after the revision, it was more painful on the right side. This was not a miracle fix for me. Again, I was uplifted by the stories of other mothers; I tried to be patient, continued with the stretches, and kept correcting shallow latch-attempts.
 Around three weeks, I started to feel a shift. One thing I have done since the very beginning with Ezra was talk him through our nursing sessions. Although this may seem silly, as in our family we already decided our dog is smarter than our baby (for now!), there is evidence that shows babies can learn when moms talk to them ( parent–infant synchrony, or affect synchrony). The left brain is the technical, watch-the-clock, math side, while the right is the emotional, easy-breezy side. It isn't really possible to get our babies to learn algebra or memorize a linear sequence of events, but it is possible for babies to absorb behaviors and coping strategies connected and displayed by their mothers or other caregivers. It's like a baby's first positive self-talk -- I let him know, not only with words but also with emotions and facial/body language, how we can improve our relationship. It can't hurt, right? I am not attributing our breastfeeding success entirely to this concept, but I feel it certainly can't hurt!
 Laid-back breastfeeding enables face-to-face interaction Laid-back breastfeeding enables face-to-face interaction How this looks: When Ezra would latch well, I would praise him and relax and smile. If his latch needed adjustment, I would say something like, "Okay, let's try that again. Open you mouth wider so it doesn't pinch." The most fun for talking and nursing was in a laid-back position while I was on my bed. I would lie in bed and prop Ezra's upper half on my upper half, with his legs basically standing on the mattress. Babies have about 20 reflex responses that kick in when they are on their bellies as opposed to their backs, and one of these is called, aptly, "stepping." As Ezra would step to get closer to the nipple, reaching it chin first and then latching over the nipple with his upper jaw, his upper lip would naturally be in an ideal position to flange open. We were also en face, ready to engage and exchange smiles, head bobs, and happy eyes. By four weeks (two days ago) I could safely say I believed we were cured. So inappropriate in an essay, but I feel that statement deserves a smiley face. This is where I go all Dorothy on you to figure out what I learned from my journey: 1. Find support. It wasn't until I connected with the Facebook group that I found experienced, real-life helpers in my area. Not only was this beneficial in assessing our situation, it also led me to the best practitioner for the job. If you haven't already met with an IBCLC experienced in ties, a group like Tongue Tie Babies Support would be a good place to ask for referrals in your area.
2. Get a second opinion -- and a third, and a fourth -- until you feel your gut agrees with what the professional is telling you. You have inner wisdom -- use it! Everything we are told is filtered through someone else's perception and experience. The first idea to pop into one practitioner's head may not be the same thing to pop into another's. In healthcare, the difference between wrong and right can sometimes be a simple difference of opinion. 3. Don't judge a book by its cover. And don't let your healthcare practitioner do the same. This means, the appearance of the tie/s shouldn't be more important than how the tie/s affect breastfeeding for mom and/or baby. The first doctor we saw (who was also an IBCLC) said Ezra's tongue-tie did not look severe, but due to the clicking, sliding, and pain, warranted treatment. If your practitioner doesn't value function over form, you may want to seek another opinion. 4. Continue to work with your baby patiently. It stands to reason the longer your baby has nursed with the tie/s, the more time he may need to get to a better place after revision. Resolution of the ties themselves is only the first part of the process; for continued progress, stretches help avoid reattachment that could come with normal healing. Your baby may also need to relearn how to breastfeed with this new and improved equipment, and that is where working with an experienced IBCLC can be integral, as well as getting bodywork done for your baby. I also chose to do tongue exercises with Ezra that are found in Breastfeeding Answers Made Simple: "Walking Back on the Tongue," and "Pushing the Tongue Down and Out."
5. Add your baby to your dental insurance. Or, be prepared ahead of time. It may just be me who makes that mistake ever, but still, I wish someone would have reminded me of that 4 weeks and, oh, 3 days ago. :)
So in April I had a baby -- a sweet, gorgeous, pink little baby. He is my fourth baby, fourth boy in fact -- and what a scrumptious, squishy baby he is. I love him. We named him Ezra.
Out in the world and on my chest, I soon began to see if he would nurse. And he did. Victoriously. I was happy, and he was happy. My midwife and I watched as his tongue passed his lower gum line and came out of his mouth, and we both hoorayed, "He's not tongue-tied!" I have not previously had a baby who was tongue-tied, but my sister has, and it was a lot of trouble to get diagnosed and treated.
Fast forward to day three: it's 10:00 at night. I am perched at my computer, Ezra screaming on my lap as I watch how-to-latch videos through tearful eyes. Each extra-pink nipple bears a horizontal stripe of raw, rubbed openness coupled with tiny scabs, and with every suck, I tighten and cringe and cry. I hate this. I label him. He is a bad nurser.
At this point in my life I have logged 11 years breastfeeding 3 different children. I have been a peer-breastfeeding counselor for 10 years. I have a pretty well-rounded knowledge of all-things-breastfeeding, both experiential and educational. I have helped countless women in similar situations figure out how to better nurse to ease or eliminate pain. And here I sit, alone at my computer, because he just can't do it right. Because he is a bad nurser.  Does this look like a good latch? Because it's not! Does this look like a good latch? Because it's not! Being new to the area, I don't have a clue who would be a good person to call for help. I left an army of good friends and trusted resources -- IBCLCs, LLL Leaders, midwives, doulas, and nurses -- years in the making. Okay, troubleshoot: I try dragging the nipple down his face and over his nose. I try teacup hold of the nipple. I try the "flipple." I try laid-back breastfeeding/biological nursing. I keep my finger taut to the nipple to try and push/shove it further back into his mouth. I try asymmetrical latch, symmetrical latch, sideways latch, and all-around-the-clock-face latch ("would you, could you in a tree?"). I even have my husband buy me a nipple shield and we try that (incidentally, that seemed to hurt even more, as Ezra couldn't latch to the shield so he would just chew my silicone-covered, damaged nipple). Nothing works, for weeks.
I was still in great pain, but the physical damage to my nipples was not getting worse, and that made me
hopeful. I found some Hydrogel Pads I had gotten as samples once, and they helped with the healing. I figured out by latching him in football hold, nursing sessions became bearable. We would also nurse lying down at night, turning on a small light to latch, stopping to make him try again when it was really, really painful (because it was never not painful). I kept looking for answers for my bad nurser.
Aside from the pain I was dealing with, Ezra gained weight exponentially; at one stretch between weigh-ins, he gained 38 ounces in 21 days. He did spit up a lot, like a lot A LOT -- overzealous amounts of milk, often flying out of his mouth in arching streams of stinky frothiness. Keeping the nipple in his mouth was difficult, as it would constantly slide out unless I held my breast in place. Once in a while when the nipple neared his lips, this disgusted look would appear on his face, as if I had presented him with something rotten and spoiled, and he would slowly chew his way up the nipple to latch. And as he nursed, he clicked like a horse trotting on pavement.
Armed with a digital camera, I took pictures of this baby every day for sport -- ahh, the joys of the Digital Age! When he was 3 weeks old I was scrolling through the latest batch, and suddenly, there it was: Ezra was crying, eyes shut, mouth open, with a tongue that curled and cupped up. Wait, I have seen that tongue before! That's a posterior tongue-tie (PTT)! Soon after birth I knew Ezra had a thick labial frenum (upper lip-tie, ULT), but I didn't feel this was the root of our pain; one of my other babies had one and it wasn't an issue, so I dismissed it without investigating the anatomy of his mouth any further. Once I saw this picture and that light went on, I began searching online, I posted the picture on Facebook to an IBCLC friend, and my thoughts about this baby shifted: Maybe he's not a bad nurser!?
 I found Cathy Watson Genna's website incredibly helpful ( http://www.cwgenna.com). We had met a few years before when she was a keynote at our local breastfeeding conference, and I decided to share this picture with her. She used the term "stingray tongue" to describe his posterior tongue-tie (PTT). From her site I found a link to practitioners around the country who diagnose and treat tongue-ties. I called to make an appointment at a clinic about 90 minutes away and was scheduled about 3 weeks out. Although I have been working with breastfeeding moms for ten years, I had not heard the term "posterior tongue-tie" until about three years ago; even then, I had not helped a mom with a PTT -- it had all been hearing and reading others' experiences. When we spoke of tongue-ties, we meant anterior tongue-ties, the obvious tethered (often heart-shaped) tongue, easy to spot, that could be clipped in a simple office procedure. While lip-ties I was familiar with, there still wasn't a lot of focus on it other than just getting babies to flange their lips out to latch. By the time we met with the doctor (pediatrician and IBCLC), I was certain Ezra had an ULT, PTT, and high-arch palate; all three of my suspicions were confirmed. This doctor agreed to fix ( release or revise) the PTT but is not a believer in touching upper lip-ties. By using scissors, a diamond-shaped cut under the tongue would give it more mobility and hopefully make breastfeeding better for us. We had Ezra at home with a midwife, and as such, I chose to decline the Vitamin K shot. This doctor wanted him to have that shot first as PTTs tend to bleed more than anterior TTs. Ezra also had a cold with an impressive cough, so it was decided we would make an appointment to have the procedure done at a later date. I left satisfied with the diagnosis and proposed treatment. While waiting Ezra's cold out, I was hooked into an amazing network of parents and professionals who have experience, knowledge, resources, and often a unique understanding of all-things-tied-in-the-mouth: Tongue Tie Babies Support Group on Facebook. There I have learned not many professionals know how to identify ties (especially PTTs); not many professionals believe in correcting ties, especially in infants; not many professionals believe ties can interfere with feeding, speech, digestion, etc. I have seen that many different kinds of professionals treat ties, from pediatricians to dentists to ENTs and GPs -- there isn't one kind of doctor who specializes in this area, it seems to be more about education and awareness than specific training that would come with a particular area of study. While some doctors fix ties with scissors, others prefer to use lasers. Some breastfeeding moms notice immediate relief and change, and others report it took weeks for things to feel better. Having more information and more time to think, I began to second-guess taking Ezra back to the doctor we saw. It had been brought to my attention by many people that Vitamin K, at this point, is most likely unnecessary because of his age. And I learned I might have dismissed the role of Ezra's ULT a little too quickly; at the time I didn't think to ask about the Vitamin K and the ULT as I was a bit overwhelmed by my crying baby and the (unexpected, male, older) resident shadowing the doctor as she examined not only my baby, but also my breasts. I found a second choice, three and a half hours away, where the treatment is done with a laser; not only could we get the PTT taken care of, we could also have the ULT revised as this doctor (a dentist) does both. I am not sure what to expect, but I am hopeful this is the right step for us...our appointment is next week.
 This is long! Be warned!
I think when a person in is a position to serve a woman while she is in labor, that person should have required training every few years, like a recertification, on what it feels like to have a baby. I am not certain how this certification could be obtained, virtual reality plus some sort of pregnancy suit? Actually having a baby? I haven’t figured out the logistics, but I have recently had a recertification of my own, and that is called, my fourth child.
This fourth pregnancy was a surprise. Technically, I got pregnant at a time when no one would be able to get pregnant – only I guess more like I got pregnant at a time I felt I was highly, highly unlikely to get pregnant. My last menstrual period was June 10th. I did not get pregnant until July 13th at the earliest (a time when I was waiting for my period to start), to July 20-ish at the latest; looking at the date he was born now (April 6th), July 13th seems closer to the target date…we were on vacation.
I had lots of irritable contractions combined with irritable baby movements (probably more of the latter versus the former) that would happen around 10 pm to 1 am. The week before labor began I pretty much experienced these every night and I hated them. During these times, I would have waves of panic and anxiety about the reality of actually having to go through the birth process again, and I was always grateful when they were over and I could finally climb into bed.
Friday the 5th of April was pretty normal except I had two very serious bouts of grumpiness that made me feel deeply in touch with someone who was (hopefully!) going to start labor soon -- it was like total,
irrational, not-triggered-by-much anger that switched on so fast, I knew it was something else with some other root than just me being moody.
We had pizza for dinner, and like I had for the last week, I restrained myself from eating too much (“If labor starts tonight I don’t want to be too full,” was my rationale). I had two pieces and then cut myself
off. I took a little nap in bed, which I hoped would actually be “going to bed,” but I woke up at about midnight when I couldn’t ignore the antics of Wild Baby any longer. I watched TV a little and sat on the ball to try and bounce my guy into a calmer state. At 1 am I decided to watch the last episode of Mad Men on Netflix so I would be ready for the new season, with the intention of going to bed after that.
At 2 am, just when I was settling into sleep, I realized I was contracting, and these contractions felt different. They came 5-6 minutes apart, were totally manageable, and lasted about 40 seconds. I tried to sleep, but I was also mindful of needing to recognize true labor so I could get my sister and my mom on the road from two and a half hours away if this really were it.
Everyone was asleep, and as long as I was okay, I felt no need to wake them. I was feeling hungry, so I ate half a lemon Chobani (again, not wanting to eat a lot) in the morning quiet. I did call my sister at 3 am to let her know it was go-time. I labored longer, in the quiet of my living room, tending to small errands and tasks between contractions. At 4 am I woke Brad up to tell him I was in labor. He came out to the living room and asked, “What can I do?” and I immediately answered, “Take the recycling out, it’s driving me crazy and I have contemplated doing it myself for the last 2 hours.” I was hoping he would just lie back down on the couch and snooze a little, but he was up and ready to go.
I thought I would wait to call my midwife until 5 am, but at 4:30 my contractions began to get stronger and longer and closer together, just as they should, and I finally had some show. I phoned Linda to let her know I was in labor. She asked me a few questions, and then said she would be over soon. She lives about 40 minutes from us.
At 6 am, Linda arrived, and things were beginning to feel real. We had our tub set up in the dining room and I was feeling a pull to climb in, but I didn’t want to stall labor if I wasn’t that far along. I asked Linda to check me and she said I was 3 centimeters (“Not quite active labor!” I thought with a little disappointment), about 90% effaced, baby maybe at -2 station? I can’t remember that part. I mentioned I wanted to get in the tub, but I should probably try the shower instead (so gravity could keep helping my labor), and Linda agreed.
I got in the shower, and I really don’t know how long I was in there. The water felt great on my belly and during contractions I would swing from side to side so the water could fan over me. In between contractions I alternated putting my foot up on the side of the shower to lunge, in case my baby was posterior like his two brothers before him. Soon I found I had to vocalize during the contractions. I was in the bathroom alone and I had a lot of time to think. The thought that kept coming back to me was, “All is as it should be,” which was part of a prayer Brad had said earlier in the week when I was feeling really overcome with fear. I rubbed my belly and talked to the baby and told him to hurry, it all felt like it was happening in slow motion.
When I got out of the shower it was about 7 am and Linda checked me again. I was 5 centimeters. I went straight for the tub at that point, dropped my towel, and climbed in.
Jacob and Jonas were awake and had been for a while. Soon Isaac woke up and came straggling out of his bedroom in his standard sleeping attire – undies and a t-shirt. Brad told him we had company and he might want to put clothes on. Before Isaac woke up I remember Brad asking Jonas if he knew why Linda was at our house so early? Jonas admitted he didn’t, and we made a joke about Linda just coming for an early-morning visit. Brad then said, “Your mom is going to have the baby today.”
I looked to the tub for the relief it had brought in the past; with both Isaac and Jonas I got into the Jacuzzi tub at 5ish centimeters and after an hour was at 9ish centimeters, and I was hoping for the same, with the addition of having the baby in the water. After 30 or 40 minutes it seemed the tub wasn’t going to work as I had planned. I had intense pain in my lower abdomen to the point of not being able to sit in a relaxing position, so the whole time I was in the water I had to be on my hands and knees, and I didn’t want to stay that way much longer. Also, Brad started making pancakes in the kitchen.
At about 7:45 my mom, sister Shiela, and her two boys arrived. I headed to my bedroom, finished with the tub. Linda had set things up around the pool in preparation of a water birth, so some rearranging was in order, moving things to my room, getting equipment ready if needed. Once in my room it was just Linda, my mom, Shiela, and I. Brad had the boys going with pancakes and if they were making any noise, I sure didn’t hear it.
I asked someone to bring the piano bench into my room as I was laboring standing up, and I wanted to continue to lunge in case I had a malpositioned baby (which I don’t think he was, but I was a little gun
shy).
I think I had Linda check me again, and I think I was 7 centimeters? I am not really clear on this part. I wasn’t ready to sit down, so I continued to labor standing up. Shiela was a super doula – she would squeeze my hips during my contractions, and it brought so much relief! One thing I know about that double-hip squeeze is, it is hard to do when you have to press your arms together at the height of a woman’s hips – you get tired fast, and the laboring woman usually doesn’t want you to stop. If the
mom can get on her hands and knees on the floor, you can squeeze her hips with your own inner knees by straddling over her back, but I didn’t even want to try or offer that as I didn’t feel good in that position.
Over and over, a contraction would come, and I would tell Shiela, “Hips, hips, hips,” and she would start
squeezing.
In reality I have no idea what kind of time span this all happened in, I say over and over, but maybe it was only about 5 contractions? Or maybe it was 10?
I did finally sit on the bed for a bit. I remember taking my watch off and handing it to Shiela with the feeling that this was taking too long. I know for a fact I wasn’t looking at my watch or paying attention to how long it was taking in a linear fashion, but it was more some sort of symbolic resignation that I
would try to just flow with the timetable my body and baby presented even though I am as impatient as they come; in the last picture of me with my watch on, I see the time is 8:55 am.
I decided to visit the toilet. I spent a couple of contractions there, and Shiela was with me. She said my noises changed and she knew I was getting closer. As I sat laboring on the toilet, I opened the shower door next to me and contemplated getting back in -- I was looking for anything to comfort me at this point. Then I decided to see if I could feel anything inside of me, so with one finger about one knuckle in I was shocked to find something! “Is that a head?” I asked. But then I realized it was a bulging bag of water, with a head behind it. After all the years of hearing practitioners say, “I feel a bulging bag of water” (which I did remember Linda saying when she checked me last), I finally knew what that felt like and what it meant. I think I almost gingerly hopped off the toilet at that point, feeling remotivated.
I had one contraction standing up, with Shiela at my hips. Then I had another, and my water exploded all over the floor. There was a little meconium but Linda said it looked old and there was no reason for concern. I finally climbed into bed.
At this point I knew it would soon be time to push. I suddenly had the need for Brad to come and be with me, so I called to him and patted the side of the bed next to me, I just wanted him to sit with me and be near. Shiela was on the other side of me, and Linda was at the foot of the bed. My mom was by the door, ready with the camera, and the boys were in the living room playing Legos (again, I never heard anything from the boys, and there were 5 of them. Actually, I think after they ate pancakes they walked to the park with the dog to play for a bit. But I do know when the baby was born, they were playing Legos in the living room).
I did begin pushing at some point, and Linda said I still had a rim of cervix and she was going to try and move it, and I was totally fine with that because if anything was holding this baby up, I wanted it gone. So for a couple of contractions she worked on that and I guess it went away. I was pushing with such intensity but it felt fruitless. I truly felt nothing moving or changing and I imagined pushing forever
and not making any progress. It was at this point that I remember thinking, “I should have gone to the hospital so I could have the drugs!” (Interestingly enough, when I had my babies in the hospital, I never thought to ask for drugs, because I know if I had had the thought, I would have asked; maybe at home when it is not an option, my brain safely went there, just as a way to cope and vent.) Brad and Shiela were helping me pull my legs back during the pushing. Instead of rolling my chin to my chest, which I have helped women remember who-knows-how-many-times, I arched my head back against my pillows. I also had my body twisted in some way, crooked a little. Linda gently reminded me to get better aligned (with words and heart I could understand at that point), while giving me positive encouragement for this task I had to undertake.
Linda! What else could you want from a midwife? Really, not one thing. As a doula, I get really uncomfortable when people say, “Stacie, I couldn’t have done it without you.” Because, come on, you could have, and you would have. I don’t want anyone’s birth experience to have me entangled as an
essential ingredient; it should be all about the mom and her family, not me. But I have to concede that
when the right person is helping you with the right words and attitude and presence and spirit, it helps make the experience even more amazing, if that is possible. When you have the right midwife, the feeling is similar to being in your own home – the comforts of being in your own bed, using your own bathroom, lunging on your own piano bench – Linda was a natural extension of that. It felt right that she be here, in our home, unobtrusively watching over the birth of our baby.
The support Shiela gave me was also invaluable. Family members don’t always make the best doulas.
Shiela actually has taken a DONA-doula training, and that coupled with what she knows about me (just about everything), made her perfect for the job. She stayed by my side, she gave me verbal encouragement, she wished she could help me more. The truth of the matter is, only the mother can have the baby, but she doesn’t have to be alone while she is having her baby. I will forever treasure that my sister was there to support me during one of the most intense experiences of my life.
Pushing was hard, it was really hard – it seemed harder than it ever had been. I know I was lost in my head, and in there, the storm was raging. Every push came with screams, I hate to say it. I have never screamed with any of my other babies. And also, I cried, which was something new for me. In hindsight I probably could have pushed more effectively keeping those screams to myself, but they just came out. I know the boys didn’t appreciate the noise (although they all later admitted they weren’t scared), I am thankful my neighbors didn’t call the police, and the screaming is not my favorite thing about the birth video – oh well!
After so much pushing (again my sense of time is really off here), finally his head emerged. I felt his head with my hand, but it really didn’t mean anything to me, I just wanted the rest of him out! I pushed for one or two more contractions, maybe three, and then his shoulders popped and he tumbled out on a
wave of fluid and tons of baby poop. Linda helped bring him to my chest, all the while rubbing him and talking to him and watching him carefully. I was so relieved and instantly went from that person experiencing the very hard work of pushing toward a goal, to that mother experiencing her baby
for the first time. I was rubbing him and toweling him off and just taking him in, my body relieved of the burden with the prize in my arms. He was born at 9:42 am.
We all watched as he turned from purple-y to pink. His apgars were 8 and 9. Very soon after birth he wanted to nurse and he seemed to know just what he was doing. The boys peeked in one by one, only appearing mildy interested (we had two 13 year olds, two 11 year olds, and one 7 year old), and then backing out of the room again.
There were lots of things in the birth kit we didn’t use. My perineum didn’t need massaging, which Linda was prepared to do. We didn’t need the bulb syringe to suction the baby’s airways. There are lots of Chux pads that didn’t get used. Everything just happened easily and well, as it so often can when left to its own devices. I am sure the level of comfort and security factored into that for me as well. I am still struck by how ordinary things were and how extraordinary they were. Within a couple hours I was back in my shower. A little while later I threw a load of laundry in. My mom bought donuts and I happily ate three. Our new (nameless) baby was being admired and touched and held by his cousins and brothers and dad and aunt and grandma, while also nursing and visually taking in all he could. In many ways it was like a normal Saturday morning at home, but then, it was also like some rare, high holy day, calm with introspection, peace and joy.
Ezra Christian was 8 pounds, 1 ounce. There was much debate about his name – the other choices were Benjamin, Ruben, and Abraham. He was born on what we in the LDS religion believe to be Christ’s birthday, and also the day the LDS religion was restored; Christian is my brother’s middle name, and we
felt it appropriate for Ezra as well.
Moving through that birth, I didn’t feel alone. I remembered so many births and situations and strong mamas moving gracefully through this work. I could name each and every one that came to mind, but hey, this one’s my story. Just know if I have been with you for the birth of your baby, you were with me during mine in spirit and endurance and admiration. This has brought me so much more appreciation and compassion for birth and women while experiencing it – that’s why I feel there should be something birth workers can do every few years to get back in touch with what it can really be like to physically grow and have a baby. It changes you, and sometimes we forget that.
 Brian Patrick Brian Patrick I am currently 37 weeks, 6 days pregnant. This means, like Arnie Grape says, "I could go at any time." In the past have I ever gone this early? No. But two nights this last week I started having irregular contractions in the evening -- more than those warm-up Braxton Hicks, but less than what I deem to be "true" labor. And it has given me a little bit of anxiety as to the realization that yes, someday soon, this baby will have to come out.
I have taught families about birth for years! I have touted the benefits of minimal-intervention during birth as long as mom and baby are okay. I have been excited for birth, pledged my allegience to birth, shared my mammalian theories about birth, and basically been on fire for the wonders birth can bring -- simply from a new, sweet baby, all the way to that complicated glimpse into what we are capable of as women. Birth has been my world -- it has been something I believe in, something I put my faith in, and something I have experienced as an incredible part of being a woman.
Yet here I sit, getting heart flutters and panic, as I experience a contraction that feels a little stronger than normal. When I get those nagging self-doubts or scary flashes of fear, I push them right out of my mind -- I can't even entertain them. If I had business with them, if there were something fruitful to come from their company, then there would be a purpose in having them hang around. But I know this much about myself: Negative thoughts are part and parcel to my brain and its chemistry, and they mostly have no function to fulfill.
To counter my own inclination of dwelling on the negative, I have found some solace: When I think about the women I have supported during their own experiences of birth, I find my confidence in birth being rebuilt.
There was Karen, who birthed her second son at home in a horse-trough-looking tub, all 12 pounds, 2 ounces of him, like nobody's business.
Amanda, who exercised her right to attempt a vaginal birth after cesarean (VBAC) in a local hospital; she walked into the hospital (no wheel chair for her!) at 7 centimeters open and soon after birthed her baby in a squat, close to the floor (I don't know if she even sat in the bed at all before the baby was born!).
Kim, who had her baby in the car on the way to the hospital with just the support of her husband.
Tara, who labored at home with a walk to Jamba Juice while she and her husband shared the story of how they met years before, as co-workers, at that same Jamba Juice (he snuck a kiss in the walk-in fridge!). Their baby was born a few hours later, peacefully and in the water.
Another Tara, who labored hard for almost two days to bring Brian Patrick into the world, on St. Patrick's day, no doubt, after being thisclose to having a cesarean birth.
Leah, who didn't let her fears get in the way of the hard work that birth is.
Kim, who was on bed-rest -- she ate breakfast, had a conference call for work, realized her water broke, went to the hospital and had a baby within an hour, had a follow-up call from someone at work regarding the conference call, and then had Thai food for lunch!
Laura, who experienced the worst kind of tragedy during pregnancy which she used for strength to have a home-water-VBAC -- I will never forget the words she kept chanting during transition, "The only way out is through. The only way out is through."
There are so many more. I remember them all. One thing I will say about birth -- no matter how you have a baby, no matter where you are or what your personal experience will be made up of, birth is a day of hard work. Regardless of whether a woman has a spontaneous, normal birth, an epidural, a cesarean birth (or whatever combination), it is generally not a day at the spa. But one thing I have always said, it is mostly a mind-game: You can psyche yourself up or you can psyche yourself out. I, for one, am working on the former, and I am so grateful for all those families who have allowed me to witness their power and strength, because right now, that's exactly what I need.
Ever since I had enough experience to help another doula out, I have been happily engaged in growing doula sisters. My first hospital birth in Chico found me in the fortuitous position of working with another doula; this was an invaluable experience. She was able to show me the ins and outs of the hospital, where to get snacks for the mom, which drawers held the pillowcases (and that we were able to access), how to get to the cafeteria -- all stuff that would have taken a lot of time, energy, and bothering-of-nurses (while I was also trying to support a family during labor). I am grateful to that doula for taking me under her wing -- I wasn't new to birth, but I was new to this hospital -- and her willingness to share her craft and her knowledge is a true sign she believes in the work doulas do.
It can be hard to find sucess as a doula -- it truly takes a village to get yourself and your name out there to the point of receiving referrals, interviews, and ultimately, births. Many women who attend doula trainings later "drop out" because they have such a hard time trying to integrate into their local birth world. In pondering this, a lot of thoughts have come to the surface which may be helpful to that doula-in-training who is about to fall by the way-side.
When we think about who might need a doula, often we focus in on our closest social networks -- our close-tie connections -- family and friends we know well. We have emotional connections with these people, we see them often and have shared past experiences with them. This can be met with gleeful agreement and anticipation on the part of these close-tie relations, or it may not get us anywhere. What can be more fruitful than this group is the next social network outside this realm -- these are known as our "weak-tie" connections.
The idea behind weak-tie connections was proposed by Stanford professor Mark Granovetter in 1973. The basic idea is the more links we have with people who are not closely associated with each other, the more opportunities we will have in business, spreading ideas, and joining together for a common cause. "Individuals with few weak-ties will be deprived of information from distant parts of the social system and will be confined to the provincial news and views of their close friends," Granovetter said. Basically, if we stay within this close-ties realm, we stifle our opportunity for further exposure to grow and branch out of our little corner of the social-world.
How does this apply to doula work? Get out there and network! Start with your close-ties and work into weak-ties via your connections. Let your close-ties know your doula endeavors and be sure to encourage them to pass on your information to people they think might have a need or common interest. Just today I virtually met a doula who lives in the town where my sister-in-law grew up and still has many friends and family -- I promised this doula I would pass her information on to my close-tie, thus providing her (hopefully) with some weak-tie opportunities that may prove beneficial at some point. Other places to find weak-ties as a new doula: church, school, clubs, the gym, work, your doctor's office, commujnity meetings and events or fairs. When you open your eyes to the potential right outside your direct family and friends, the possibilities are not only endless, they can also be much more promising.
 I am not sure if you know this or not. With your first pregnancy it may come as a surprise -- with subsequent pregnancies it is an easy thing to forget until it creeps up on you, but it gets terribly uncomfortable growing a baby who sits on top of your bladder and underneath your rib cage. I have long told my childbirth classes this, and as of late, I am reminded again of its truth.
Being 33 weeks pregnant, I have my list of complaints. I feel like this baby can't come fast enough. I even imagine going into labor early -- like today early -- just to be done with it.
My back and hips are aching like never before (surely a sign my body is feeling too old to be going through a pregnancy again, right?). Sleep is something that comes in fits and pieces. I feel bad for my husband as I toss, turn, try to roll over but feel more like Ralphie's brother in "A Christmas Story," lying on the ground in his snowsuit saying, "I can't get up!" Add to that restless legs that shake and quake of their own volition, the 5 pillows I have behind, around, under and between various body parts, and the snoring (yes, the snoring!) that wakes me -- the snorer! -- and I imagine there's nothing peaceful in our bedroom right now.
My baby is still high enough that I can relate to this scene from "Tommy Boy," just replace bear claws with baby butt:
It is surprising how hard a baby butt can actually be -- but there is not a lot of fat there, and it becomes this firm blockage that prevents me from bending over to put on socks or tie my shoes or reach down to release the emergency brake on the car -- and it is just plain uncomfortable.
Even with the baby still not having "dropped," my poor bladder is being pushed to its own limits. I am convinced I am currently the top toilet-paper-user in the house, visiting the bathroom 4-5 times a night, and so many times during the day I probably use a roll every 24-hours. I have adopted a policy of mandatory-usage if I get within 12 feet of a bathroom. My logic is, even if I don't have to go right now, I will in 10 minutes, so I just pre-emptive-strike it.
I notice I make a lot more noises as I progress through the normal tasks of the day. I sigh and groan and yelp as I shift from sitting to standing, getting in and out of the car, bending down to (attempt) tying my shoes. I swear I am not doing it on purpose, these sounds just escape my lips before my brain can even say, "That was quite the old-lady-carrying-the-cat-food-bag-into-the-house noise." No offense to old ladies who have to carry the cat food bag into the house and may make noises while doing so.
This baby gets the hiccups probably 6-8 times a day. I can't figure a pattern -- sometimes it seems like they may come after I eat, other times they come when I am hungry. Sometimes they just come. They aren't the worst things in the world, they just feel like lttle spasms that jolt my uterus in various places every two seconds. They can space out longer or shorter, but in my scientific explorations, I have noted they most frequently come every two seconds.
These are just the things that bother me the most. There are more issues I can mostly overlook. With this list of complaints, though, it isn't hard to see why so many women press for inductions or agree to inductions when offered. It is hard to wait! It is uncomfortable to wait! It pretty much sucks! Don't believe that rare woman who, at 38 weeks pregnant says, "I still feel great, I am in no hurry to be done," because while she does exist, she is generally the exception, not the rule.
The way we look at due dates, we often feel "overdue" by the time that day rolls around. We are conditioned to believe our (bad, uncooperative, lazy) babies are just kicking back in there, buffing their ever-growing nails on the inside of our uteri, taking up time and space, while we grow more and more uncomfortable.
When I was pregnant with my first baby, I read in "What to Expect When You're Expecting," that doctors only induce if it is medically necessary; so when my doctor offered, on my due date, to induce me, I took her words as medical advice being as they came from my medical practitioner's mouth. Maybe my first clue should have been the way she asked without giving any scientifc rationale: "Are you ready to get this over with?" Well, heck yeah, I was ready to get this over with! That's a vulnerable place to be! Miserable, anxious, wanting that baby out from under your ribs and into your arms. Who would say no? And with that one question, I was set up to believe my body was done doing anything important for my baby and wouldn't go into labor on its own.
I am not a patient person. I hate waiting for things. It took every ounce of confidence and trust I could muster, and some I didn't even know I had, to wait on my babies and pregnancies the next two times around. But the evidence shows birth is safer for mom and baby when they are allowed to work together -- like Mario and Luigi saving the princess in tandem -- to let labor begin on its own.
 I had a cavity filled today. I like my new dentist, he is a funny guy and his
staff is friendly -- they remember my name. My dentist was chatting today about when he was a kid, he was always building things. He decided he wanted to be an engineer, but once in school, a fellow engineering-turned-dentistry-student talked to him about becoming a dentist, and he changed his mind. "I like being a dentist, but sometimes I think I should have stuck with engineering." From my stand-point, or chair-point (lounge-point?), I see the fields of dentistry and engineering as pretty similar -- bridges are built in both, right? He seems to think we should write a book together, about something important, I guess -- the topic is still undecided.
I had a lower cavity filled, and my dentist made sure I was good and numb -- actually, my whole tongue was numb and half of my lower jaw, including the right side of my lip. After he injected the medication, he asked me to keep my mouth open for a couple of minutes and to stretch the muscles, and also tilt my head to the right so the anesthetic could gravitate downward to provide better coverage. Once he came back, and I could take the spit-sucker out, close my mouth, and then open it to talk, I shared with him that when a woman receives an epidural a similar anesthetic issue can occur. After epidural placement, a woman is propped on her left side, and if everything is going well, she is left in this position indefinitely. Gravity causes the medication to pool into that lower left side, leaving the right side less-anesthetized. Have you ever heard from a woman, "My epidural only worked on one side"? This could
be why. My dentist agreed this made sense.
There are ways to prevent this, something called "pancake-flipping," where we have the woman lie on her left side for a few contractions, and then we help her move to her right side for a few; next we facilitate a forward/hands and knees position, usually with lots of bunched-up pillows. As mom keeps "flipping," it helps to evenly distribute the medication through her lower body.
I wanted an epidural with my first birth -- I had voiced that request loud and clear for months before I even had a hint of what labor would feel like. In my case, I never received one. In hindsight, I am glad for that, but at the time I was bitter. Regardless, today I felt like my tongue had epidural anesthetic. (I realize, just as there isn't a specific "epidural" drug, it is a cocktail of different medications that can be changed according to an anesthesiologist's preference and a patient's needs, "epidural" refers to the specific spot where the medication is placed -- the epidural space is the sac of fluid that surrounds the spinal column. Obviously this doesn't apply to my tongue.) My dentist requested I move my tongue to the left so he could drill on my tooth a little. I tried to move my tongue, but I was unsure if it was actually going anywhere! "I can't tell ith I am moothing it or not!" I half-mumbled, half-dribbled. I was instantly reminded of being with a past client who had a heavy epidural, during her pushing phase, and the doctor demanding, "Push! You need to push!" To which her confused reponse was, "I can't tell if I am pushing!?"
I do like my dentist, he is gregarious and puts me at ease; I think I will, however, give him six months to ponder over what we could collaborate on -- I am in no hurry to return back to the chair to get an epidural for my tongue.
|
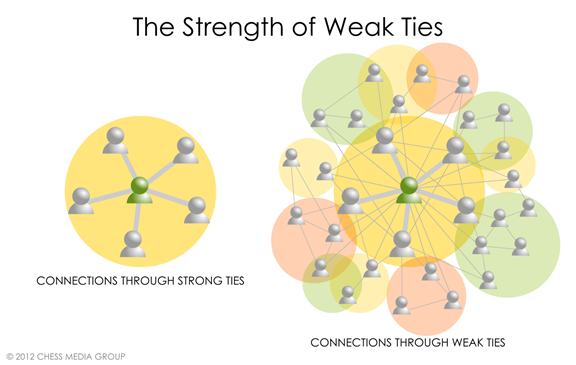
 RSS Feed
RSS Feed