The Cascade of Interventions is a typical topic covered in childbirth classes. I don't want to say it's like the Domino Theory of Communism,a logical fallacy known as "slippery slope," but it...it kind of is. As moms, doulas, educators, and birth workers, we often can recall someone's "cascade of interventions" story. The important thing when it comes to teaching is to help students understand that the use of an intervention doesn't mean a woman is fated to the "next" likely step -- with education and awareness, she and her partner can be work to avoid the common pitfalls a specific intervention might bring. Basics:
The story I use:
The bolded statements are being recorded on a large sheet of paper as we read along. After the activity with the boxes, we go through the list and discuss what can be done to avoid or minimize the effects from a specific intervention. This is also the time I hand out basic info sheets about common interventions.
I hope I included everything? If you have questions, ask! And please "like" my Facebook page to stay up-to-date on the teaching tips I share.
- I like to use story-telling in many childbirth education activities. Roger C. Shank, a cognitive scientist, said: "Humans are not ideally set up to understand logic; they are ideally set up to understand stories." I feel this is an effective way to help participants relate and remember bits of information, versus throwing factoids at them.
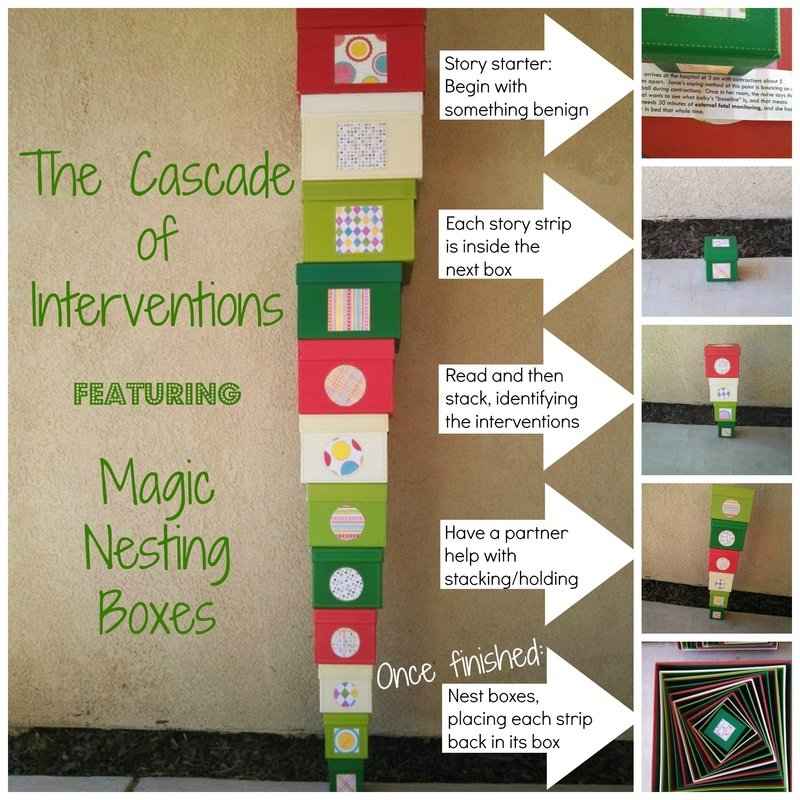
- I have a set of 12 boxes, that when stacked reach over my head (and I am 5'5"). I bought them at Costco about 7 years ago with this activity in mind.
- I have a 12-step story with each step written on its own slip of paper. The first part of the story is in the smallest box. Step two is in the next size up box, etc. I put these under students' chairs before class.
- Parents offer their boxes as size/story dictates, read their part of the story, then stack their box. In reverse-size order we see how even though the small box was no big deal, as the stack increases, it starts to teeter, and it might even fall. I ask a partner to be in charge of holding the stack up while we finish the activity.
- This story starts with the tiniest box in my nesting collection, and it is a benign "intervention," one we might not even consider when looking for offenders: external fetal monitoring. The story ends with breastfeeding being interrupted -- of course the worst thing we generally think of within the context of normal birth situations is cesarean birth; I felt that was an obvious choice. When it comes to cesarean birth, I feel it can be easy for participants to think, "That won't be me," whereas breastfeeding interference seems an idea we can open our ears to.
The story I use:
- EFM: Jamie arrives at the hospital at 3 cm woth contractions about 5 minutes apart. Jamie's coping method is bouncing/swaying on the ball. Once in her room the nurse wants to get a reading on her baby and requests 30 minutes of EFM to get a 'baseline" on baby.
- limited mobility; increased pain/anxiety Jamie's limited mobility means she is no longer able to sit on the ball through her contractions. Her contractions become more intense, and this starts the F/T/P cycle.
- pain medication request (Stadol) Jamie is scared about how she can cope with labor if it is going to get worse. She decides she wants to try an analgesic pain medication, which can be given as a shot.
- labor stalls Jamie finds although the medication takes away some of the pain, her labor has stalled.
- pitocin to speed things up; IV Jamie now needs pitocin to get into an active labor pattern. This means she will have an IV as well.
- epidural request As the pitocin increases the strength of her contractions, she experiences F/T/P cycle again. She requests an epidural.
- blood pressure drops Jamie's blood pressure drops in response to the epidural.
- medication for blood pressure Jamie gets meds to counter low blood pressure.
- maternal fever Jamie has a fever, which could be from the epidural.
- OFP affected; baby born via vacuum Since Jamie was not able to be more active, her baby has not had help moving and rotating into an optimal position and needs the vacuum to be born.
- baby has fever; sent for observation, possible septic work-up Baby has a fever at birth and needs to be taken to the nursery for observation and possible tests. Jamie and her baby are separated for 6 hours.
- separation/breastfeeding affected Breastfeeding is affected.
The bolded statements are being recorded on a large sheet of paper as we read along. After the activity with the boxes, we go through the list and discuss what can be done to avoid or minimize the effects from a specific intervention. This is also the time I hand out basic info sheets about common interventions.
I hope I included everything? If you have questions, ask! And please "like" my Facebook page to stay up-to-date on the teaching tips I share.

 RSS Feed
RSS Feed